How to feed & monitor for feed intolerance in a LBW infant?
In this webinar, we shall learn how to feed and how to monitor for feed intolerance in LBW infants.
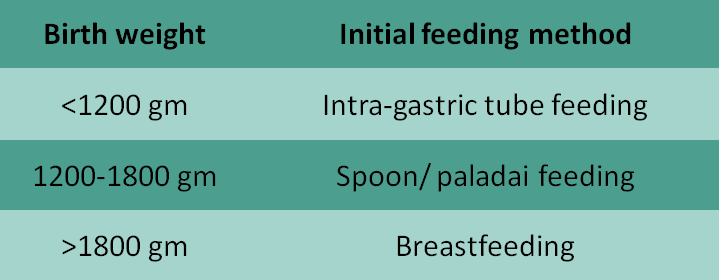
The preferred initial feeding method in LBW infants is usually decided by their feeding skills. Roughly, the feeding skills correlate with gestation and birth weight. As a rule of thumb, any baby with birth weight <1200 gis initially started on Intra-gastric tube feeding. Babies weighing between 1200 and 1800 g are started on spoon or paladai feeds while those weighing >1800 g are given direct breastfeeding.
But these are only rough guidelines – a baby with birth weight of 1700 g baby may be able to feed directly from the breast – in which case, there is no need for spoon feeds.
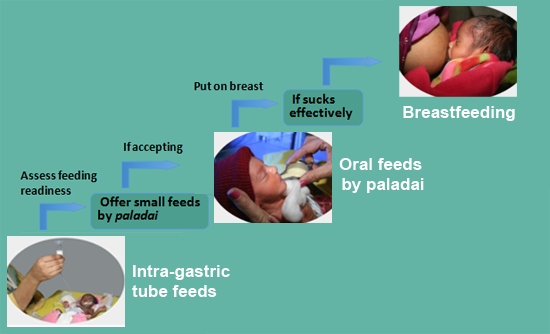
All LBW infants should ideally be on direct breastfeeding by the time of discharge from the hospital, irrespective of the initial feeding method. They must be assessed periodically to check if they are ready to accept BF. For babies on Intra-gastric tube feeds, the feeding readiness should be assessed daily. If ready, they must be offered small feeds by spoon or paladai. If they accept well, the amount by spoon can be slowly increased to reach full paladai feeds. Babies on full paladai feeds should be put to breast daily. They should be assessed for effective sucking at the breast. If they can suckle effectively for adequate time, direct breastfeeding should be initiated.
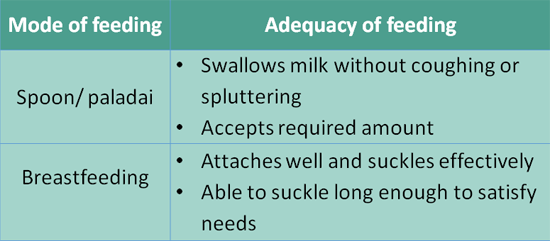
Babies on any mode of feeding – including intra-gastric tube feeding – should be assessed for adequacy of feeding on a regular basis. If the baby is on spoon/paladai feeds, adequacy is indicated by the following criteria: Baby swallowing milk WITHOUT coughing or spluttering, and Baby accepting required amount of milk. Babies on breastfeeding are said to be feeding adequately if: They can attach well and suckle effectively; and they can suckle long enough to satisfy needs. For all modes of feeding, other indicators of feeding adequacy include. Adequate weight gain – 15 to 18 g/kg/d after 7-10 days of birth; and Passing urine at least 6 times in 24 hrs
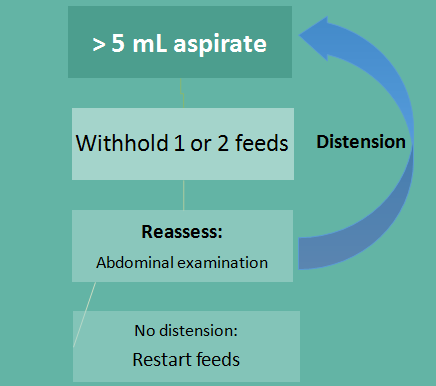
All LBW babies should be assessed for feed intolerance by careful inspection of the abdomen before EACH feed. If there is obvious abdominaldistension,the stomach contents should be aspirated to check the nature and volume of aspirate. If the aspirate is clear but is more than 5 mL, the feeds should be withheld for 1-2 feeds, after which we should reassess by abdominal examination.
If there is no distension, we can restart feeds. If there is distension, we should aspirate the contents again and then decide.
If the aspirate or vomit is Bile or blood-stained, feeds should be withheld for 24-48 hours. The babies should also be evaluated for local and systemic causes like NEC. We can restart feeds after 24-48 hours depending upon the abdominal and other systemic examination findings. Thank you
- Introduction...
- 1. How to feed?...
- 2. Progressing fro...
- 3. Assessing adequ...
- 4. Monitoring for ...
- 5. Monitoring-01...
- 6. Monitoring-02...
 |
 |
Introduction
DR. M JEEVA SANKAR
MD, DM (Neonatology)
Assistant Professor
Department of Pediatrics
AIIMS, New Delhi
1. How to feed?
2. Progressing from initial feeding method
3. Assessing adequacy of feeding
For all modes:
Adequate weight gain; passing urine
6 times in 24 hours
4. Monitoring for feed intolerance

5. Monitoring-01
6. Monitoring-02
